Article Text

Abstract
Objectives To explore the experiences of women living with HIV in England who received or gave Mentor Mother (trained mother-to-mother) volunteer peer support during pregnancy and early motherhood.
Design Qualitative descriptive study, using semistructured, in-depth interviews and inductive thematic analysis, theoretically informed by phenomenological social psychology.
Setting A London-based third sector peer support organisation for people living with HIV.
Participants 12 women living with HIV who had given or received Mentor Mother volunteer peer support (6 had given support and 6 had received support). 11 were black African.
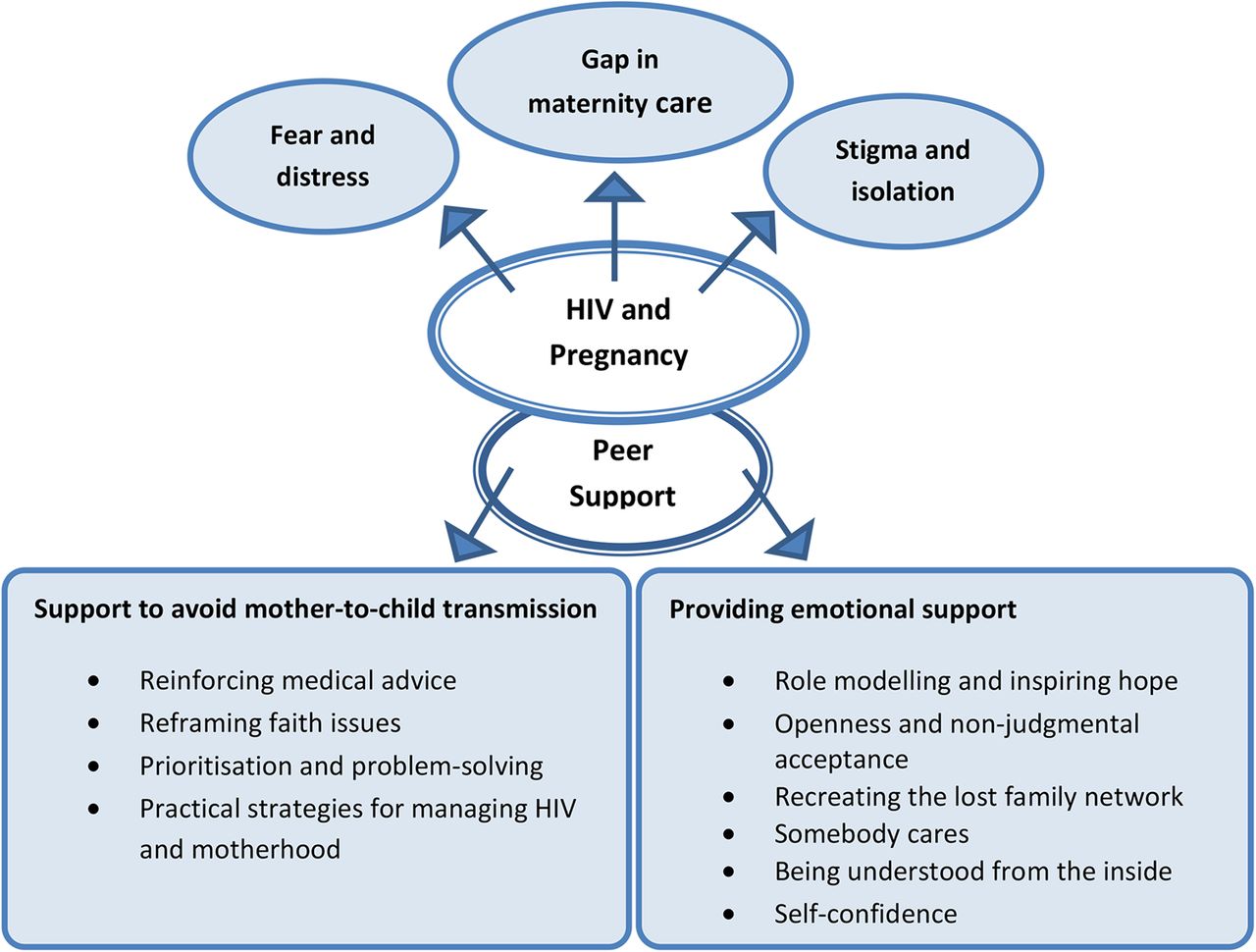
Results The key themes in participants' descriptions of their lives as pregnant women and mothers living with HIV were ‘fear and distress’, ‘stigma and isolation’ and ‘the gap in maternity care’. The key themes related to Mentor Mother peer support during and after pregnancy were ‘support to avoid mother-to-child transmission’ (with subthemes ‘reinforcing medical advice’, ‘reframing faith issues’, ‘prioritisation and problem-solving’ and ‘practical strategies for managing HIV and motherhood’), and ‘emotional support’ (with subthemes ‘role modelling and inspiring hope’, ‘openness and non-judgemental acceptance’, ‘a caring relationship’, ‘recreating the lost family network’, ‘being understood from the inside’ and ‘self-confidence’). The Mentor Mothers' support appeared to be a successful hybrid between the peer education Mentor Mothers programmes in southern Africa and the more general pregnancy volunteer peer support models operating in England.
Conclusions A Mentor Mother peer support programme is acceptable to, and valued by, black African mothers with HIV in England. Peer support from trained volunteers during and after pregnancy can complement and reinforce medical advice on avoiding mother-to-child transmission of HIV, and can have a multidimensional positive impact on vulnerable mothers' emotional well-being. Mentor Mother peer support should be considered by those designing programmes for the support of pregnant women with HIV and the prevention of mother-to-child transmission of HIV.
- HIV
- peer support
- pregnancy
- Mentor Mother
- qualitative
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first in-depth study of the experiences of women living with HIV and involved in Mentor Mother volunteer peer support in England.
This study enables the voices of a very marginalised group of women with complex needs to be heard.
Consistent with other in-depth qualitative peer support studies, the number of participants was small.
Participants were contacted through the project co-ordinator so the researchers were not aware of how many declined to participate or whether they differed from those who took part.
Background
Screening for HIV is part of routine antenatal care in England with 98% uptake of the screening test. In 2013, 2.5 per thousand pregnant women tested positive for HIV, of whom one in six were newly diagnosed in pregnancy.1 The risk of mother-to-child (vertical) transmission of HIV can be greatly reduced if the mother takes antiretroviral therapy (ART) during pregnancy, gives birth by planned caesarean section and has intravenous ART during delivery if her viral load is high, formula feeds the baby from birth, and gives the baby ART for several weeks after birth.2 The rate of mother-to-child transmission of HIV in England has fallen from 25.6% in 1993 before treatments were available,3 to <2% in 2006–2012.1 Where the mother was diagnosed and treated, the transmission rate was just 0.46% in 2010–2011.4
The majority of pregnant women living with HIV in England are black African, with HIV affecting around 2–3% of pregnant women born in sub-Saharan Africa, compared with around 0.5 per thousand women born in the UK.2 Research on the experiences of black Africans with HIV living in England consistently highlights the shock and fear associated with HIV diagnosis, and the subsequent struggle with stigma, resulting both in feelings of shame because of the cultural associations of HIV with promiscuity, and social isolation in an attempt to conceal HIV status from the African diaspora communities.5–7 Black Africans living with HIV often experience social problems connected with insecure immigration status, including poverty, poor housing and dependence on abusive partners.7 ,8 In this context HIV is experienced as one of a range of stressful life circumstances but not necessarily the most important one.7 ,8 Pregnant women living with HIV face additional challenges, such as the struggle to maintain a ‘positive maternal identity’9 in the face of diagnosis, guilt and fear about their babies' safety, and the need to lie about why they are not breastfeeding.9–11
In England, the ‘Standards of Care for People Living with HIV’ recognise that peer support ‘enables people with HIV to develop confidence and gain information and skills from others’.12 International evidence affirms the beneficial impact of peer support on knowledge and attitudes to HIV,13 although the definition of where the boundaries of peer support lie is still evolving.14 A peer support model for pregnant women with HIV was developed in South Africa in 2001 and has since spread to other sub-Saharan countries. ‘Mother2mother’ or ‘Mentor Mother’ programmes train mothers with HIV to provide support and advice to pregnant women with HIV, and are successful in increasing women's confidence in their ability to prevent vertical transmission and improving their adherence to prevention guidelines.15 ,16
Small scale volunteer peer support programmes for pregnant women and new mothers outside the context of HIV are well established in England17 but Mentor Mother peer support specifically for pregnant women with HIV in England is new. This qualitative study explores the experiences of mothers with HIV who were peer supporters or had received peer support in England's first Mentor Mother project. It forms part of a larger qualitative study of peer support for pregnant women and new mothers in England, aiming to understand the impact and dynamics of peer support from the perspectives of those giving and those receiving support.17
Methods
Study design
This was an qualitative descriptive study,18 using semistructured, in-depth interviews, informed by the theoretical perspective of phenomenological social psychology,19 and underpinned by contextualism.20 This ‘low-inference’18 design was chosen because the aim was to explore participants' own perceptions and lived experiences, while acknowledging the role of both participants' understandings and the researchers' interpretations in the production of knowledge21 and the researchers' responsibility to ground findings closely in participants' experiences.22
Both researchers are White, UK-born women with children. They worked reflexively, sensitive to the potential impact on participants of talking to an ‘outsider’ researcher from a different cultural background and whose HIV status was not declared, and putting aside prior knowledge and experience so that data analysis remained close to participants' accounts.
Setting
The setting was Positively UK, a London-based third sector peer support organisation for people living with HIV. From 2012–2015, Positively UK ran a Mentor Mothers project, which trained women with HIV who had a child to offer one-to-one peer support to pregnant women and new mothers with HIV. These ‘Mentor Mothers’ received 36 hours of training for their unpaid volunteer role, leading to an accredited qualification; the training included both core training on peer mentoring techniques and specific training on HIV in pregnancy. Pregnant women needing support were usually referred to the project by HIV specialist healthcare professionals, and were paired up with a Mentor Mother by the project co-ordinator (the women supported by Mentor Mothers are referred to as ‘supported mothers’ in this paper). Where possible this pairing process took account of language, cultural background, length and experience of HIV diagnosis and the complexity of the supported mother's needs. The Mentor Mothers gave support through telephone calls and face-to-face meetings, and the intensity and length of support varied according to the woman's needs (it could begin before or during pregnancy, and continued as needed after birth). Mentor Mothers received regular supervision and support from the project co-ordinator.
Data collection
Between June 2014 and April 2015, 12 women with HIV who had given or received peer support took part. The researcher first met the project co-ordinator to describe the research. The co-ordinator explained the research to the project's 10 active volunteers and to the recently supported mothers using the study information leaflets and asked their permission for the researcher to contact them, or arranged with those who wished to participate when the researcher could interview them. The sampling was thus purposive insofar as all participants had experience of giving or receiving peer support while living with HIV. The researcher arranged to meet each person who decided to participate at a time and place of their choice (a 13th woman who had initially agreed to take part dropped out at this stage because of a change in personal circumstances).
After giving written informed consent, participants took part in a semistructured qualitative interview which explored their experience of giving or receiving peer support and of using maternity services. Topics for supported mothers included: their involvement with the peer support project, the impact of peer support and their feelings about the voluntary nature of the peer support and its ending. Topics for volunteers included the training, peer support activities, support received from the project, the impact on supported women and the impact on the volunteer. Two interviews were carried out by telephone at the participants' request, and informed consent was taken orally and recorded. Data collection continued until saturation was reached in the themes identified in the analysis.
The interviews were audio recorded (range 30–86 min, median 43 min) and fully transcribed. To protect anonymity, each participant was given a unique identifier beginning ‘MM’ for Mentor Mothers and ‘SM’ for supported mothers.
Data analysis
The interviews with the Mentor Mothers and supported mothers were analysed as separate data sets, using inductive thematic analysis.23 Each transcript was checked against the audio recording, then read and reread. Codes were identified inductively and recorded using NVIVO software. Codes were refined as data collection continued, and emergent themes identified; the technique of constant comparison24 was used to reconsider earlier codes and emergent themes. Themes emerging from each data set were compared. To ensure the validity of the analysis, each researcher independently analysed the transcripts, and codes and emerging themes were discussed and agreed.
Results
In this section, some results are described for ‘Mentor Mothers’ and some for ‘supported mothers’; the term ‘participants’ is used where the results include data from both Mentor Mothers and supported mothers. Some results are identified as coming from all participants and some from a subgroup (the 11 black African participants).
The participants
Six Mentor Mothers and six mothers who had been supported by a Mentor Mother took part. Eleven of the participants were black African, all first generation migrants from Guinea, Malawi, Nigeria, Uganda and Zimbabwe; one Mentor Mother was black British. Eleven participants had between one and three living children, and one Mentor Mother was planning her first pregnancy; three participants had experienced the death of a baby; and one of the living children was HIV positive. The participants ranged in age from their late 20s to early 40s. The Mentor Mothers had known their HIV status for 6–23 years and supported mothers for 1–12 years. Two participants had been diagnosed with HIV during pregnancy. Four participants were in work, three were unemployed and five were not allowed to work because of their immigration status.
The black African participants had experienced a range of challenging circumstances apart from their diagnosis with HIV, including the death from HIV/AIDS of a partner, child or family members; separation from children and family left behind in the country of origin; uncertain immigration status; domestic abuse; rejection by their partner; poverty and homelessness. The Mentor Mothers had all received peer support from other women with HIV before they became peer supporters.
Participants' accounts of living with HIV
There were three key themes in the 11 black African participants' accounts of living with HIV: ‘fear and distress’, ‘stigma and isolation’, and ‘the gap in maternity care’ (these themes were not reflected in the black British Mentor Mother's account). These themes are shown in figure 1.
{kind=link}
Themes and subthemes arising from analysis of pregnancy, peer support and HIV.
Fear and distress
The participants described their shock and distress on being diagnosed with HIV: ‘It was like heavens going to fall’ (SM05); and some distanced themselves from HIV by speaking euphemistically: ‘this thing’ (SM04); ‘my condition’ (SM06). Pregnancy created an additional level of anxiety, specifically worries whether their baby would be HIV positive and whether they would survive to bring up the child. Some experienced severe mental distress on discovering they were pregnant: ‘Sometimes I just cried nights, sometimes I think of committing suicide … . Am I going to look after this baby? What about if the baby is positive?’ (SM02).
Stigma and isolation
Participants had made great efforts to hide their HIV status because they were keenly aware of the stigma within diaspora African communities: ‘My people … the moment they see you they'll start talking, back biting, “Oh don't go near her, that one she is HIV positive”’ (SM06). Some had actually experienced discrimination when their HIV status was discovered: ‘Nobody wanted to go in the toilet anymore…they would sneer at me,“Oh you are dirty”’ (MM12). One participant described how stigma made it difficult to access information about HIV and pregnancy:‘HIV is just swept under the carpet, you know? Some [pregnant women] might not want to take the literature with them for fear of maybe some member of their family, they will discover that they are reading about HIV and there will be the question, ‘Why are you looking at HIV?’ (MM10)
Fear of gossip, and a desire to protect family ‘back home’ from distress, had led most participants to try to keep their diagnosis secret from family and friends as well as the community: ‘My immediate family…I don't want [them] to go,“Oh, she's got this thing, she's going to die.” …And my extended family, they will just go round telling everybody’ (SM04). Most participants had no supportive partner relationship, and disclosing their HIV status to their partner had for some led to the end of their relationship or triggered an escalation of abuse: ‘He's using my HIV status to talk at me, I'm HIV lady that are going to die soon…Everything little thing I said, the message is he must slap, beat me, and the other day he said he is going to kill me’ (SM03).
The gap in maternity care
All the supported mothers said they had received excellent antenatal care from specialist HIV midwives and obstetricians. However, they felt that health professionals did not have time to answer questions or address anxieties: ‘The midwives…it's always because of their time. Sometimes they just check on the baby and then they will tell you a little bit’ (SM02); or that they followed their own important, but restricted, medical agenda: ‘They always think, only have ten minutes to get through a patient, but then they will explain everything you need to know, the things that matter to your doctor’ (SM03). One Mentor Mother noted that because survival rates had improved dramatically, health professionals underestimated the implications of HIV for the individual:‘Medical people, I feel like it's easy to brush people off now. You know, ‘There is medication, you're fine … Just deal with it and go.’ But at the same time it's a big thing, and the fact that we cannot talk about it easily like a headache, I don't think…that impact of it on individual life is going to go away.’ (MM12).
The impact of peer support
There were two key themes in the 12 participants' accounts of the impact of peer support: ‘supporting mothers to avoid mother-to-child transmission’ and ‘emotional support’. The themes and their associated subthemes are shown in figure 1.
Supporting mothers to avoid mother-to-child transmission
This theme describes how Mentor Mothers enabled women to recognise their ability to protect their babies from HIV.
Reinforcing medical advice
At the most basic level, talking to a Mentor Mother helped pregnant women to engage with the reality that they were pregnant and HIV positive, and to begin to gather information and take decisions: ‘One week they don't talk about HIV, they can't even mention the word “HIV”, two weeks they are talking to me about treatment, they are asking me about, “What tablet is this?”’(MM07). Some mothers struggled with the side effects of the medication or worried that it would harm their baby, and despite the information they had received from doctors, it was to the Mentor Mothers that they turned for reassurance: ‘The last time they gave me more medication I am not so sure about it, I was on the phone to [the Mentor Mother] straight…I so much trusted her. If she said “no” I believe that is no’ (SM02). It was very important to hear the message that ART was effective in preventing mother-to-child transmission from another mother with lived experience of HIV and successful pregnancy outcome: ‘[The Mentor Mother] was just there encouraging me, she has kids and they are okay, you should just follow everything they have told you and your baby then will be okay’ (SM06).
The Mentor Mothers reinforced the importance of following doctors' advice: ‘Be vigilant whenever they are talking. Don't just go in the doctors and think he is blabbing nonsense, no, he is talking about something very important’ (MM07); but also empowered mothers with the knowledge that if they did suffer side effects, they could ask for medication to be changed, rather than giving up on ART: ‘Sometimes it's just telling them, “I've taken some tablets whereby I had side effects, I had to go back to the doctor and say, “I am not taking it anymore.” So you have that right as well’ (MM07). Peer experience of taking medication meant that the Mentor Mothers could complement the medical advice with empathetic understanding:‘Someone who has HIV already telling you, ‘I have received this medication, I was worried taking about this medication, I understand your feeling but you need to take this.’ While the doctor is thinking about the numbers…we are thinking about the feeling about taking it, so we come from different angles.’ (MM11)
Reframing faith issues
Many of the participants had religious beliefs that could give meaning to their experience of illness and peer support: ‘At times I will say, “Oh, should I be thanking God I am positive?”’(SM06); ‘I feel extremely blessed…my being positive actually became a positive’ (MM12). However, one Mentor Mother described how some women attending Pentecostal Christian churches believed that taking ART represented a lack of trust in miraculous healing achieved through prayer. Since she shared their faith she was able to reframe the issue appropriately to persuade them that there was no inconsistency between taking ART and their beliefs:‘Some people think, ‘If I take medication that means…I am not having enough faith.’ … You just tell them for example, like Jesus, he was a healer and when he was healing this blind man he prayed for him and…made a paste of some mud and smeared him in his eyes, and I take that as medication…I talk about this in line with my faith.’ (MM09)
Prioritisation and problem solving
Some mothers had been so overwhelmed with other crisis issues that they had not focused on their medication: ‘At that time there was a whole lot going on, and the HIV was the least of my problems… I was homeless…sleeping on the buses… I am pregnant, baby was coming anytime, there was no money’ (SM04). Mentor Mothers responded by helping the supported mothers to break down their problems into separate issues and to resolve them, for example by supplying secondhand baby clothes to those who had no money, or referring to other organisations who could support them with food, formula milk and advice on housing or immigration: ‘[We take the problems] one at a time, and then we solve that, we go to the next one’ (MM07). This practical problem-solving was greatly appreciated by mothers: ‘Everything is easier now [because of] all the help I get from them’ (SM06).
Mentor Mothers did not ignore mothers' own priorities but asked questions, to challenge their perceptions of the relative importance of different issues and highlight the time-critical necessity of taking ART in pregnancy even if they were preoccupied by other difficulties:‘We are not here to give them answers or to force them to do things the way we want them to do, but to ask them the right question so that they can think of it and come to us and say, ‘No, this is really what I want.’ …So we have to work with them for them to see what is really important … It's really sometime you wake them up… [They say,] ‘I don't like medication, the side effect and everything, but I have to protect my baby.’ (MM11)
Practical strategies for managing HIV and motherhood
Unlike professionals who were perceived not to have the experience to deal with ‘the nitty gritty stuff’ (MM09), Mentor Mothers addressed practical concerns about motherhood and HIV by sharing what had worked for them, for example how to manage giving babies medication: ‘You can relate to the person sharing…you'll be like, “Why don't you try this? I've tried it, it works for my kids.” And the social worker is not going to tell you that’ (MM08). In particular this centred on hiding clues about HIV status, for example, excuses for not breastfeeding, and how to take medication discreetly in shared accommodation: ‘You can talk to them about medication, about how to tell other friends who are not positive why you are not breastfeeding’ (SM01); ‘You just normalise the way she takes the medications… having water all the time by the bedside so that nobody suspects why she is bringing water into the room, why can't she drink it while everybody is looking’ (MM09).
Emotional support
This theme describes the multifaceted nature of the emotional support that the mothers received from their Mentor Mothers, and the reciprocal effect on the Mentor Mothers.
Role modelling and inspiring hope
There could be a powerful emotional impact on a pregnant woman simply from meeting a Mentor Mother who was living with HIV, and yet who was well:‘Up to that moment, despite all the talk I still believe that, ‘Oh, anybody that has HIV is going to die.’… I didn't know that [the Mentor Mother] is positive… I was like, ‘Why is this woman smiling? She didn't know that it is a dead body, a living corpse that is sitting in front of her now.’ Then when she narrated her story, she told me that… twelve years now, she has been positive.…She made me understand that…everything is going to be okay.’ (SM05)
As well as inspiring hope by role modelling successful outcomes, the Mentor Mothers gave mothers the confidence to disclose their HIV status and problems by trusting them with their own disclosure: ‘Everybody who hears your story of what you have gone through…the next day they are a different person, they feel like, “If she has gone on with it, I think I can deal with it as well”… They are free to talk about everything ‘cause they feel like, “Okay, she has told me her own story, why shouldn't I?”’ (MM07). One mother described the emotional impact this made in life-or-death terms: ‘I don't think if I didn't go to [Positively UK] I would be alive up ‘til now’ (SM02).
Openness and non-judgemental acceptance
Mothers described how the culture of secrecy around HIV had made them unable to discuss their fears about motherhood with anyone else: ‘You need to talk to someone… you will be thinking, “Maybe I'm alone in this world who is facing this problem”’ (SM06).They therefore experienced an enormous release through talking frankly with a Mentor Mother: ‘You feel more open, you feel more free to ask any kind of questions’ (SM01). Crucially, peer support was a non-judgmental relationship in which the mother could be accepted while being fully herself: ‘If we were judging it would be like judging yourself as well’ (MM09); ‘You don't have anything to hide…[they] accept you for who you are’ (SM04). Being accepted by another person could lead onto self-acceptance: ‘When other people say it's okay, you start saying it's okay’ (MM12); and this enabled mothers to begin to build positive emotional relationships with their unborn babies: ‘They are beginning to accept the virus and beginning to cherish the time they are pregnant. And you can see that they are looking forward to the newborn baby as well’ (MM07). It could also have a reciprocal effect on the Mentor Mothers: ‘The more I've shared with other people… I feel lighter. So for me it's a healing process as well… it's a two way thing’ (MM12).
A caring relationship
The socially-isolated supported mothers described how feeling that someone really cared about them had boosted their emotional well-being: ‘Just knowing somebody was concerned about me’ (SM04). The fact that the Mentor Mothers were proactive and made themselves available flexibly contributed to this sense of genuine emotional connection: ‘She would call me without even an appointment just to check on me…I used to say “Oh God, that's good”’ (SM02); ‘If I flash her she's going to call back, “Are you are okay?” Even though you call her out of her comfort zone” (SM03). Some mothers felt cherished because Mentor Mothers gave their own time as volunteers: ‘It was really good…she is not paid and sometimes maybe you call her…and she will leave what she is doing and she attended to you” (SM02). However, one mother felt inhibited from asking for all the help she would have liked, because she did not want to impose on her volunteer: ‘I just feel that she is a mother and she has got two little kids so I didn't want to disturb her most of the time’ (SM01).
The Mentor Mothers emphasised that this sense of connection was real for them too: ‘It's more personal …there's a bond’ (MM08); and it was very rewarding: ‘To see a woman call me…and say, “Thank you, you don't know what you have done to my life”’ (MM07). It could also be emotionally challenging, because some supported mothers were in upsetting situations: ‘At certain times you are choked and you want to maybe cry’ (MM09); this was partly because mothers' stories could bring back memories of their own experiences: ‘They are always at a very low point and it just brings back all that I felt’ (MM08). Some Mentor Mothers experienced distress that they could not do more: ‘I have felt hopeless because the woman was going through so many things… and I didn't have enough time to solve it’ (MM11). These Mentor Mothers both recognised the importance of the boundaries of the peer support relationship, and struggled to maintain them: ‘Sometimes you feel incredibly responsible beyond a point that makes any sense’ (MM10); but they felt supported by the organisation in managing their feelings: ‘You have to have boundaries. But at times you really want to go beyond… We have people we can see and talk about it’ (MM11).
Recreating the lost family network
Most of the supported mothers and some of the Mentor Mothers used the language of ‘family’ and ‘home’ to describe their mentor relationship and the peer support organisation: ‘Like a mum’ (SM02); ‘Like a sister… like a home’ (SM03); ‘A whole new family’ (MM09). In situations where mothers were cut off from their own families, it appeared that the Mentor Mothers were practically as well as emotionally filling some of these roles: ‘Like a biological mother…anytime I had the hospital appointment with my midwife, if I gave her a call she can be there for me, and I can even invite her to be my labour partner’ (SM01).
Being understood from the inside
The empathetic understanding that the Mentor Mothers had for clients was framed as underpinning the emotional support they provided: ‘The mothers that I work with, they are all going through things that I've already been through—the abuse in a relationship, the partner leaving you, the immigration, the being homeless, the having no food and everything. So having been there, I can empathise better’ (MM08). This made them able to offer support very sensitively: ‘I try not to push too much ‘cause the one thing I have to remember as well is when I first found out I was HIV, was I ready to deal with it?…So I have to be really gentle and just let them know that I'm there’ (MM08). The supported mothers also felt the impact of this peer empathy strongly: ‘[The Mentor Mother said] “You can even call me anytime, even if you talk something which is not sensible, just call me, I will understand”’ (SM06).
Developing self-confidence
Since the Mentor Mothers were a trusted source of information, they could help pregnant women gain confidence in their ability to understand options and make choices: ‘She told me everything, when I went to labour I really knew what they are going to do…it was like it wasn't new to me’ (SM02). The Mentor Mothers saw their support as having a natural progression from intensive to occasional as women grew in their self-belief: ‘When they are starting we see their emotion or confidence, they are one, zero, two, three. [Later] you ask them the questions and they are all tens’ (MM07). This confidence could be experienced as liberation from fear: ‘I'm happy and I'm proud… this is how a person [is who] doesn’t have something to control them’ (SM03).
The black African Mentor Mothers also described how volunteering had transformed their own self-esteem and self-confidence: ‘I'm okay with my HIV. I can talk to anyone about it… Everything about me is changed’ (MM07); ‘I feel so empowered to see how far I've come…Not just to be now a service user, it was a little bit of like upgrade in life… I felt like, “Oh I have got a purpose”’ (MM12). Meeting so many mothers living with HIV and having HIV negative children had changed their perspectives about motherhood: ‘When [doctors] say, “You are positive,” that's the first question of every woman, ‘Will I not have babies?’ Seeing that they are having babies is just feeling that we have beaten HIV a bit. We won at some point, it didn't stop us!’ (MM11).
Discussion
The black African mothers' descriptions of the challenges in their lives closely mirrored those of other studies,5–7 ,25 as participants highlighted their distress on being diagnosed with HIV, and the emotional isolation that resulted from trying to keep the diagnosis secret in the face of ‘felt and enacted stigma.’26 The difficulties of living with HIV were intensified by poverty, poor housing, insecure immigration status, relationship breakdown and domestic abuse. As pregnant women, the culture of secrecy had contributed to significant gaps in their understanding of vertical transmission and ART, and enormous anxiety about whether they and their babies would survive. Although they had received good antenatal care, mothers felt there were many important issues that health professionals did not address, because of the pressure on their time and because they did not understand the situation from a mother's perspective.
The Positively UK Mentor Mothers project appeared to work as a hybrid between the peer education Mentor Mothers programmes in southern Africa and the pregnancy volunteer peer support models operating in England. The African Mentor Mothers programmes focus on promoting retention in care, encouraging disclosure, education on feeding practice and some psychosocial support;16 whereas many of the English peer support projects focus on social and emotional support alongside information, support to access services and sometimes encouragement for behaviour change.17 This fusion was illustrated in the two key themes in the 12 participants' accounts of the impact of the Positively UK Mentor Mothers: ‘supporting mothers to avoid mother-to-child transmission’ and ‘emotional support’. There was an important information component, because pregnant women trusted messages about the safety and efficacy of ART medication from peers with lived experience of HIV and motherhood, more than they trusted the same messages delivered by professionals. At the same time Mentor Mothers' own stories of giving birth to babies who were HIV negative were seen as providing proof that what the clinicians said was true.
The complex role of Pentecostal Christian beliefs in relation to ART medication in England has been noted in other studies, which have found that some believers are inhibited from taking medication by their faith in divine healing, while others see ART as an instrument of divine healing.5 ,8 ,27 This study showed specific techniques a peer supporter could use to move a pregnant woman's religious understanding from an anti-ART to a pro-ART perspective.
As in other studies of black Africans in England,7 ,8 HIV was not necessarily seen as the most important problem an individual faced. Mentor Mothers helped the supported mothers to disentangle and solve their own priority issues, while at the same time asking questions that enabled mothers to realise the time-critical importance of taking ART during pregnancy. Mentor Mothers shared practical tips from their own experience, and made mothers aware of their right to ask for changes to medication if the side effects were unmanageable.
The emotional impact of Mentor Mother support could be transformational, helping mothers to overcome feelings of anxiety and depression,28 embodying hope,29 ,30 and offering a non-judgemental acceptance that helped mothers to repair their ‘spoiled identity’26 ,31 and accept themselves as HIV positive and as mothers. The key mechanisms were the Mentor Mothers' openness about themselves, their empathetic understanding and their proactive, flexible, empowering approach, which made mothers feel that they could speak honestly5 ,7 and would still be worthy of care and concern. Mothers expressed this feeling of being wholly known and yet genuinely cared for using the language of ‘family’ and ‘home’, reflecting their estrangement or physical distance from their own families.5 ,32 This kind of emotional support has a particular significance during pregnancy, because mothers' depression and stress before and after birth can have lasting negative consequences for the child's physical, psychological, mental and emotional development.33
The Mentor Mothers also described the emotional impact of their work as peer supporters. Consistent with studies of peer support in the context of HIV (but not pregnancy) in the USA,30 ,34 there were emotional challenges in supporting very vulnerable mothers (in particular distress at not being able to do more, and maintaining boundaries to the relationship), but the Mentor Mothers also experienced personal growth in self-esteem, and self-confidence through their volunteer role.
A key strength of this research was enabling the voices of very marginalised mothers living with HIV to be heard, in the first study of Mentor Mother volunteer peer support in England. Another strength was the parallel analysis of the experiences of peer supporters and mothers, enabling reflection on both perspectives. The small number of participants, although typical of qualitative peer support research, was a limitation, as was the fact that participants were contacted through the project co-ordinator—this was necessary to gain the trust of some very vulnerable women, but meant that the researchers were not aware of how many (if any) declined to participate at that stage or whether they differed from those who took part. Although the researchers were conscious that their ‘outsider status’ might affect participants' willingness to talk about their experiences as mothers living with HIV, in practice being introduced by the project co-ordinator appeared to have overcome this potential barrier to trust and all the participants freely described their experiences. Further research could explore whether the model has equal salience for pregnant women with HIV from different cultural backgrounds.
Conclusion
A Mentor Mother peer support programme is acceptable to, and valued by, black African mothers with HIV in England. Peer supporters and supported mothers powerfully describe organised peer support during pregnancy as complementing and reinforcing medical advice on avoiding mother-to-child transmission of HIV, and as having a multidimensional positive impact on vulnerable mothers' emotional well-being. Mentor Mother peer support should be considered by those in more economically developed countries who are designing programmes for the support of pregnant women with HIV and the prevention of mother-to-child transmission of HIV.
Acknowledgments
The authors are most grateful to all the women who participated in this study, to Positively UK for facilitating the research, and in particular to the project co-ordinator Angelina Namiba.
References
Footnotes
Contributors MR and JM developed the concept and research questions, designed the study, and participated in the data analysis, critical revision of the manuscript and its redrafting. JM collected the data and drafted the manuscript.
Funding This paper reports on an independent study which is funded by the Policy Research Programme in the Department of Health. The views expressed are not necessarily those of the Department of Health.
Competing interests None declared.
Ethics approval The Oxford University Medical Sciences Research Ethics Committee (reference MSD-IDREC-C1-2013-111) approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.